
Articles

There was a battle between science, business, and politics which affected the narrative of what was going on and lead to an emergence of conspiracy theories. People are growing fatigued with the situation and become increasingly concerned about their personal plight depending on how secure their income and job situation is. There is a need for addressing the psychological needs of people.
Emerging technologies (Artificial Intelligence/Telehealth) has probably reached the tipping point in healthcare industry and is here to stay. There probably is no going back to the way things were.
When it comes to survival, living in a group offers many perks, the most important one is the feeling of sense of safety and security that allows us to concentrate on making progress by not facing the threats alone. Organization leaders are reframing the dialogue using different approaches.
TAKING A PROJECT MANAGEMENT APPROACH
Projects should be judged against two parameters:
- How well defined are the goals
- How well defined are the methods
(Turner & Cochrane, 1993) created a goals-and-methods 2 x 2 matrix that defines four types of project. Organizations should use different techniques to handle the different types of projects. These different types of projects require different techniques and execution methods to be adopted. Organizations should negotiate agreement of the goals and brainstorm methods of achieving them where they are ill defined with key stakeholders, as shown in Figure 1 below.
Countries handled the pandemic situation in different ways: Some countries (South Korea) handled it as a Type 1 project with greater chance of success in controlling the transmission by clearly defining the methods (social distancing, using masks, tracking the incidence, etc.) and taking a bottom-up approach. Other countries handled it as a Type 4 project and struggled to define the methods and in establishing clear goals using more of a top-down approach (U.S.). And some countries started as a Type 4 and quickly took corrective measures and moved to a Type 1 approach.
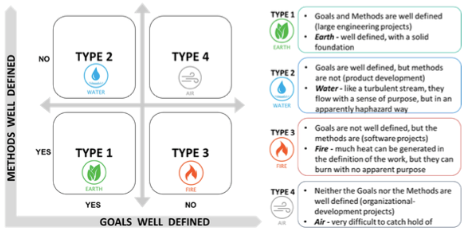
Figure 1: Goals vs Methods (Turner & Cochrane, 1993)
IMPLICATIONS
The point of this discussion is not to evaluate the effectiveness of the various approaches from a clinical perspective, but to highlight the virtues of Project Management. Of particular concern should have been the safety and morale of front-line essential workers in hospitals, food preparation, distribution, law enforcement, and the military. Project Management clearly improves employee engagement which is related to being:
- Clear about expectations
- Having the right equipment
- Getting feedback
- Feeling their opinion counts
- Having a mission/purpose they agree with
- Feeling that their role is meaningful
Essential workers clearly did not feel safe, properly equipped, or adequate compensated for the risk they were taking to themselves, and their families who they might infect.
Sweden and South Korea had clear, well defined approaches, whereas the U.S. approach was an air approach, difficult to catch a hold of in terms of goals and methods (Turner & Cochrane, 1993). The plan was constantly shifting, expectations were not clear, equipment was lacking, and the majority of people disagreed with the approach, especially around sharing information with other countries and working together. This approach also left stakeholders confused including manufacturers of supplies, testing centers, health care providers, and other nations we previously were aligned with.
If a project management approach was applied in the US there would have been a clearly defined Executive Sponsor Team, well defined goals, and methods used that were monitored through testing and data analysis and led to a greater probability of success. Without those things in place the U.S. population was susceptible to debates around science vs business, which ultimately led to conflict, mental fatigue, frustration, and an inability to objectively evaluate the outcomes.
What does this say about your own organization? How can innovative project management approach guide the mission, vision, values, and goals of your organization, given the various challenges you face?
CHALLENGES
There were various challenges raised by the participants in today’s session:
- Everyone is looking to someone else to step up and provide leadership during these chaotic times
- The corporatization of healthcare has gotten in the way of some human needs
- How do we get health care providers to see things from the patient perspective
- Who are the other stakeholders in healthcare (Insurers, pharmaceutical companies, equipment manufacturers, stockholders) and how do we address their needs
- Politics obstructs action, but how can politics be harnessed to accomplish positive things?
- How do we recognize and address racial inequality?
- What are the specific needs of the aged population who are being affected by Covid-19 at an alarming rate?
- What can we as individuals do to make a difference?
- How do we close the knowledge gap? What sources can be trusted to provide accurate information?
- How can we put a face to the impact of Covid-19; 100,000 deaths is just too large a number to grasp. These were human beings with lives that matter to their loved ones.
- We need a business case to get something meaningful done. Unless you have buy in from politicians, organization leadership, and funding sources nothing will get done
- When there is a void in leadership, it provides an opportunity to try different things
- Corporations need ways to monetize any suggested solutions
REFERENCES
Turner, J. R., & Cochrane, R. A. (1993). Goals-and-methods matrix: coping with projects
with ill-defined goals and/or methods of achieving them. International Journal of project management, 11(2), 93-102.
ABOUT THE HOSTS
| Saravana “Samy” Govindasamy is a success-driven, entrepreneurial leader with 20+ years of progressive experience in management, strategy, innovation, and technology consulting Samy has held executive leadership positions and spearheaded innovative enterprise-wide transformation programs/projects in excess of across the full continuum of care for medium and big health systems by establishing PMO/innovation centers using design thinking and agile methodologies.
Samy also possesses Big 4 consulting experience. Throughout his consulting career, Samy has built a reputation for achieving bottom line results, effectively aligning business and technology needs, and leading and developing high-performance teams for Fortune 50 global organizations. Samy’s educational background includes a Doctorate in Business Administration, Fox School of Business, Temple University, Philadelphia, USA, Master of Business Administration, and a Bachelor of Engineering. Samy holds Project Management Professional (PMP) and Lean Six Sigma in Healthcare certifications. Samy has published papers in refereed journals and has delivered professional speaking engagements in the areas of healthcare innovations, strategy, operations management, project/program management and process improvement. |
| Michael Grossman has been a nursing leader for over 40 years in a variety of clinical settings. Grossman is certified as a Nurse Executive Advance-Board Certified (NEA-BC) and Nurse Manager Leader (CNML). He has worked in a variety of roles including staff nurse, clinical nurse specialist, manager, director, coordinator of leadership development, and nurse entrepreneur.
Grossman is a frequent national speaker on a variety of topics including leadership, change, quality improvement, teamwork, and working with emotionally difficult patients and families. Grossman earned his doctoral degree in management of organizational leadership from the University of Phoenix. He is a graduate of Widener University where he received his BSN and MSN in Emergency and Critical Care nursing. He also has a BA from Temple University in Psychology. |